Olecranon fracturesThe olecranon is the corner of the elbow at the back. It is one end of the ulna and it is the ulna and the radius that make up the forearm. If one was to fall directly onto a flexed (bent) elbow, it is possible that the olecranon would fracture (break). The olecranon is important because it forms part of the elbow joint and it is the bit of bone that the triceps attaches to. If left alone there is a risk that the elbow will not bend properly because the joint is disrupted and that triceps will not be able to straighten the elbow. There are two options really when dealing with an olecranon fracture.
Non-operative treatmentIf the fracture is undisplaced (the fracture hasn’t opened up) then it may be possibly to manage the injury without surgery. Alternatively, if the patient is frail, has low demands of the elbow and is high risk for a general anaesthetic then it may be preferable to not operate. The options may be a sling with or without a plaster-cast. Elbows tend to get extremely stiff if kept in a plaster for more than a week or so.
Operative treatmentThe more usually way of managing these injuries is to stabilise the fracture with some metalwork. The two main types of surgery would be a tension band wiring (TBW) technique or a plate and screws. A TBW technique uses 2 parallel wires along which the fracture can slide. In order that the fracture slides and is compressed together, a figure-of-eight wire is wrapped around the 2 straight wires and the ends are twisted to shorten them slowly. This squeezes the 2 parts of the fracture together and usually works very well. This technique can only be used if the fracture is in a certain place on the olecranon and if there is no comminution (multiple fragments) to the injury. The other common way of managing these injuries is by using a plate and screws (ORIF – open reduction and internal fixation). The cut in the skin is made along the back and a pre-contoured (shaped) plate is placed onto the bone and the fragments held with screws. The advantage of using a plate is the pieces of bone can be held quite accurately in order for healing in the best position. If the pieces heal in a good position then this reduces, but doesn’t eliminate, the risk of stiffness. Stiffness in inevitable to some degree. The main advantage to both TBW and plating is that early movement of the elbow can commence so you may be put in a plaster for only a very short time or perhaps not at all. It is important to look after your wound well by keeping it dry for 2 weeks. Usually patients lose a little bit of extension (ability to fully straighten the elbow). However, this isn’t usually a major problem. The functional range of elbow movement is from about +20 degrees to about 120 degrees of flexion. The metalwork does not need to be removed in either TBW or plating methods. However, it is quite common for the wires used in TBW to work loose and can threaten to poke out through the skin. If this happens your surgeon may recommend the metal is removed. This would need to be done under general anaesthetic again. After metalwork removal it is usually safe to move the joint and return to normal within a few days. 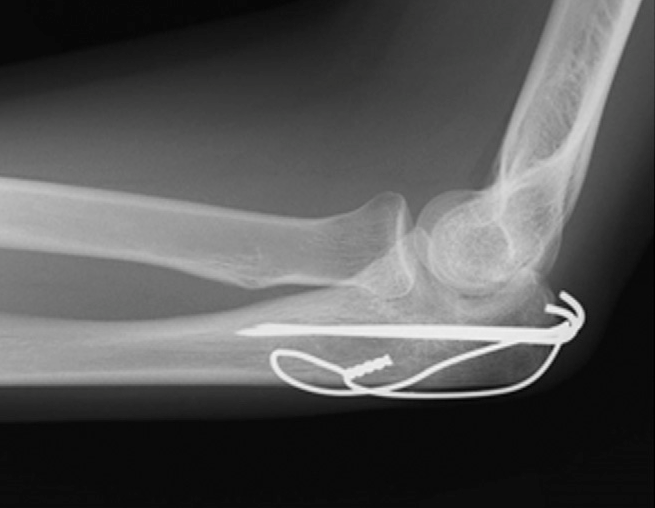 
|