WHAT IS ELBOW OSTEOARTHRITIS?Elbow osteoarthritis is wear and tear of the elbow joint surfaces which can lead to pain, stiffness and loss of function. The elbow joint is made of the junction of 3 bones: the humerus, the radius and the ulna. The humerus and (principally) the ulna form the hinge joint and the radius and the ulna allow supination and pronation (the act of rotating your hand around from palm facing the floor to palm facing the ceiling).
WHAT CAUSES OSTEOARTHRITIS?Articular cartilage is a highly specialised tissue which is smooth and supple but it can degenerate if over-worked (eg, heavy manual labour) or if damaged by trauma. If the joint surfaces are no longer lined up correctly, the cartilage will wear down more quickly than one would expect by just age alone. Worn out joint surfaces isn’t the only cause of pain in osteoarthritis. Fragments of the joint surface can become loose and break away and start to float around in the joint. These fragments are called loose bodies.
WHAT SYMPTOMS DOES OSTEOARTHRITIS CAUSE?Early arthritis may give intermittent pain perhaps only after a bout of particularly hard manual work. Loose bodies may be the first sign to the patient that there is a problem as they tend to float around and get stuck in the articulation of the joint. This can be compared to a door wedge stopping a door closing. This ‘locking’ of the joint can be very painful but usually the patient can ‘unlock’ the joint by giving a certain movement to free the loose body. As the arthritis progresses, the symptoms become more frequent or even permanent in nature. The principle symptoms are pain and stiffness. It is common for the pain and stiffness to actually improve with exercise and worsen with rest. Symptoms are typically worse in the morning and improve as the day goes on. Pain may interfere with your sleep. When all the articular cartilage is worn off the joint surface, you may begin hearing crepitus which is the two bone surfaces creaking against each other.
Stiffness tends to start as the inability to straighten the elbow, which may or may not be painful. Gradually the patient may notice the elbow also does not bend as well as it used to either. The movement whereby the hand is turned over so the palm is facing down and then up (pronation and supination) is often well preserved.
HOW IS IT DIAGNOSED?A detailed history and examination is necessary. Questions will include how long you have had the pain and how this affects your work and/or sporting or social activity. They will also ask about specific symptoms like locking and pain at night. An examination of the joint will be performed to assess movement of the joint and function of the nerves supplying the joint and beyond it. Your clinician will probably request a simple x-ray. This can demonstrate loss of the normal joint space along with bone changes associated with arthritis.
Sometimes a CT scan will be considered if further information is required, particularly if there is early arthritis.
WHAT IS THE TREATMENT?
Nonsurgical treatment:It is most sensible to consider non-operative treatments first as often simple measures can give acceptable relief of symptoms. Your surgeon may recommend non-steroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen, to help control swelling and pain. Other treatments, such as alternating heat and cold can help.
Physiotherapy can be of some benefit particularly in strengthening the muscles around the joint and improving joint control. However, it cannot reverse damage to the joint.
To improve your symptoms you may need to consider modifying or limiting your sport or activities. You may even need to consider a change of job if your work requires heavy, repetitive motions with the hand and wrist. An injection of steroid into the elbow joint can give some temporary relief. Steroid is very powerful at reducing inflammation. It can be very effective at relieving pain and swelling. Its effects are temporary, usually lasting several weeks to months. There is a small risk of infection with any injection into the joint, and cortisone injections are no exception. Also, there is a limit to the number you should have in any one joint as it could limit your option for possible surgery in the future.
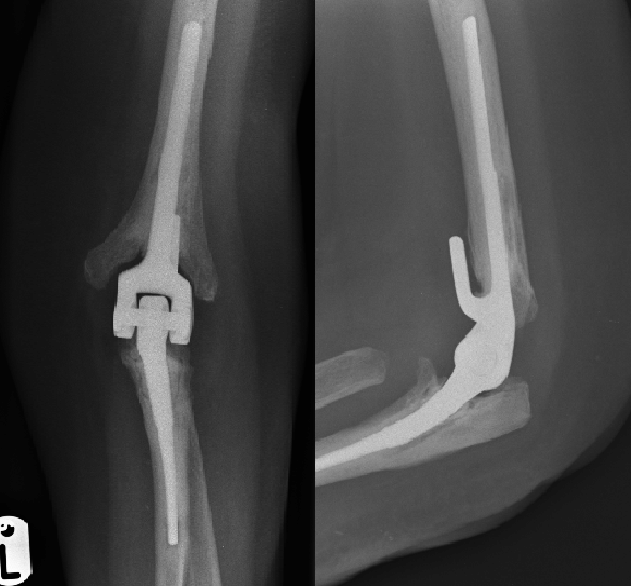 Surgical treatment:Elbow replacement surgery is not as common as hip or knee replacement. The reasons for this are, firstly that the elbow is not a true weight-bearing joint like the hip or knee. It makes sense therefore that it doesn’t wear out quite as quickly. The second reason is that it has a higher complication rate than hip or knee replacement surgery due to the amount of bone that the replacement has to support it and the amount of soft tissue (skin, fat and muscle) surrounding the joint. Nevertheless, replacing the elbow with a prosthesis (artificial joint) can be very successful in reducing a patient’s pain and improving quality of life. It is primarily a pain relieving procedure and should not be embarked upon to improve movement or strength. It is generally accepted that a patient will recover the same movement after the replacement as they had before, but no more.
After the surgery the patient is limited to lifting weights no heavier than 1-1.5 Kg (about the weight of a bag of sugar). Regular episodes lifting more than this is likely to lead to the replacement loosening within the bone (just like tiles will loosen within grouting on a bathroom wall). Elbow replacement has commonly been performed for rheumatoid arthritis in the past with good results. Due to the modern drugs available for rheumatoid arthritis now, this procedure for this indication is much less common. In the advent of GIRFT (Get It Right First Time), elbow replacement services are provided in just a few centres within Yorkshire. I do not personally offer elbow replacement and would refer you on to an appropriate surgeon.
Spire Elland HospitalElland Lane
Elland
HX5 9EB
For an appointment, telephone:
Clinic Bookings on 01422 324 069
Self pay enquiries on 01422 229 597
Main Hospital on 01422 229 632
BMI The Huddersfield Hospital
Birkby Hall Road
Huddersfield
West Yorkshire
HD2 2BL
Reception: 01484 533 131
Department of Orthopaedics & Trauma
Calderdale and Huddersfield NHS Foundation Trust
Huddersfield Royal Infirmary
Acre Street
Lindley
Huddersfield
HD3 3EA
NHS Secretary:
Mrs Margaret Thomas
Tel 01484 342 343
NHS Clinics Trauma:
Calderdale Royal Hospiatl (Halifax) and
Huddersfield Royal Infirmary
Elective Shoulder and Elbow problems:
Friday morning at Calderdale Royal Hospital, Halifax
|