ARTHRITIS
WHAT IS IT?
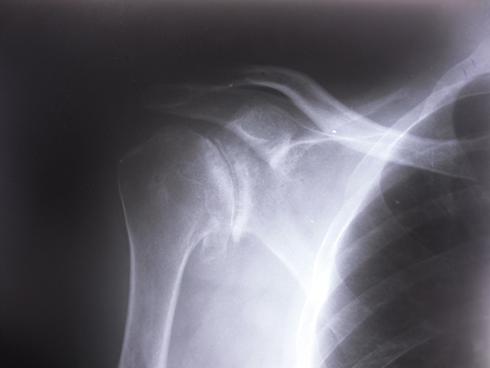 A xray of the shoulder showing arthritis. When using the term 'arthritis', it is important to establish which sort of arthritis you are referring to. Osteoarthritis essentially means ‘wear and tear’ of the joint and occurs when the protective surface (cartilage) becomes thinned and breaks down. The surface becomes very worn and uneven and this is painful and the joint feels stiff. Rheumatoid arthritis is a widespread disease found throughout the body in which the patient’s own immune system mistakenly attacks the joints causing widespread inflammation and damage. There are other types of arthritis, for example, psoriatic (pronounced sorry-attic) arthritis which is painful joints associated with psoriasis, the common skin condition. Septic arthritis is a very serious infection in a joint and needs emergency medical treatment.
There are two joints in the ‘shoulder’ which can be arthritic. The main shoulder joint (the gleno-humeral joint) is the larger of the two and is the ‘ball and socket’ joint. The second is much smaller and is the acromio-clavicular joint (ACJ) between the end of the clavicle (collar bone) and the acromion (bony shelf formed by the scapula) as it comes round from the back. This joint twists particularly when one lifts their arm above shoulder height and can become arthritic particularly in heavy manual workers or people who regularly use their arms for repetitive activity above shoulder height. Arthritis of the acromio-clavicular joint is dealt with under a different section on this website.
Osteoarthritis of the shoulder is less common than in the hip, knee, ankle or hand. However, it can still cause significant pain and since the main purpose of the shoulder joint is to position the hand for activity, it leads to major loss of function of the whole arm.
The precise cause of arthritis is not fully understood but several factors have been identified in predisposing its onset. These include a family history, previous trauma (especially fractures or dislocations) and overuse of the shoulder, eg. long term heavy manual work, weight lifting and racquet sports.
Rotator cuff arthropathy is the term that is given to osteoarthritis that occurs after long standing large tears of the rotator cuff (deep tendons of the shoulder). Although it is less common than the other forms of arthritis, it can be more disabling as the mechanics of the joint are significantly altered. Fortunately, just because someone has a large tear of the rotator cuff, it does not mean that they will necessarily progress to disabling arthritis. Indeed the majority do not develop disabling arthritis.
WHAT ARE THE SYMPTOMS?The symptoms that patients commonly experience with arthritis of the shoulder include:
Pain - which is worse on use of the arm and often associated with painful “catching” and ‘creaking’.
Stiffness – lacking the full range of movement - especially lifting the arm above shoulder height or rotating the arm, especially going behind the back.
Night pain - sleep is frequently disturbed and patients have difficulty lying on the affected side.
Loss of function - limited ability to perform normal activities, especially activities at head height, eg. reaching items out of high cupboards, doing hair etc
These symptoms generally deteriorate with time although it can be impossible to say at what rate the deterioration will be.
HOW IS IT INVESTIGATED?Your surgeon will take a detailed history and perform an examination of your shoulder. Usually a simple X-ray of the shoulder is sufficient to complete the diagnosis (see fig 9). If further treatment is planned then usually a CT scan is required. This is basically a more detailed X-ray which gives more information about the shape of your shoulder to plan the shoulder replacement.
HOW CAN IT BE TREATED?Preventative measures or very early treatment is recommended and includes maintaining a healthy body weight and remaining active to keep muscle strength from diminishing. Work up to a well-designed and well-balanced exercise program and you can keep or even improve joint flexibility. One should keep repetitive overhead activity to a minimum and rest joints only if they become very painful.
Osteoarthritis of the shoulder is initially treated by physiotherapy including exercises to maintain movement and strength. This is often combined with painkillers including paracetamol, codeine and anti-inflammatories such as ibuprofen. Your GP can advise you regarding these medications. Supplements such as Glucosamine tablets may help in early stage arthritis.
Patients who suffer from Rheumatoid arthritis need advice from a specialist Rheumatologist who can provide expert management regarding medications that can suppress the effects and progression of the Rheumatoid disease.
A steroid injection into the shoulder joint (glenohumeral joint) may give temporary benefit and relief of pain. There is a small risk of joint infection with this.
The suprascapular nerve (SSN) supplies motor function (movement) to supraspinatus and infraspinatus (important muscles in the shoulder) but it is thought to carry sensory (pain) fibres back from the shoulder to the brain. An option for pain-control in the shoulder can be injection of the SSN with a local anaesthetic and steroid. The amount of time and effectiveness of this is variable but the risks are low, and if it is effective it can offer many months of pain-relief. It is usually reserved for patients who are not suitable for shoulder replacement operation, perhaps due to pre-existing medical conitions.
If the measures described so far fail to control the symptoms then surgery may be considered.
SURGERY FOR THE SHOULDER WITH ARTHRITIS
  Picture showing anatomic shoulder replacement A keyhole (arthroscopic) debridement (clean-up) of the joint may be performed which aims to smooth off the rough surfaces and remove debris. It is likened to giving the car tyres a re-tread. It does not give you a new joint, but it can buy some time before any further procedure is necessary. Results can vary. It is most helpful when a patient is on the young side for a total joint replacement and wishes to remain very physically active.
When symptoms significantly affect the quality of life, becoming severe with constant pain, night pain and loss of function then a shoulder joint replacement is indicated. The main surgical options are to perform either a total joint replacement (both the surface of the ball and socket are replaced) or a hemiarthroplasty joint replacement (only the surface of the ball, humeral head, is replaced but the socket surface is not replaced).
One of the major concerns with all joint replacements (hip, knee, shoulder, elbow etc) is how long the joint will last. There is usually one side of the joint that is easier to fix onto the bone than the other. In the hip, the stem in the femur is easier and more securely fixed than the socket in the pelvis. In the knee, the component at the end of the femur is usually more securely fixed than the one at the top of the leg (the tibia). In the shoulder, the replacement for the head of the humerus (the ball) is usually well fixed. It is the socket (the glenoid) which tends to loosen first. This is why, over many years, surgeons have tended to only replace the head with a metal ball and do nothing with the socket (a hemiarthroplasty). We have come realise that whilst this is acceptable, patients can still experience pain from the socket-side arthritis and so patients who have an artificial socket put in tend to get greater improvement in their pain. These patients though have the added risk that the socket may loosen requiring revision (repeat) surgery.
The cut in the skin for the operation is usually about 15cm long and is on the front of the shoulder. Any remaining cartilage is removed and either a cap is placed over the existing ball or the existing ball is removed and replaced with a ball on a stem (all metal) which is placed down the canal of the humerus. The stem and ball is about the size of an ice-cream on a cone. The socket is plastic and is either fixed to the bony socket with cement or screws. The surgery takes about 1-2 hours and after the surgery the arm is in a sling for 6 weeks to allow the wound and tendons to heal. The arm can be removed early on however for light activities below shoulder height, elbow exercises and for washing and dressing. In order to access the shoulder during the surgery an important muscle must be detached and then repaired at the end. This muscle (subscapularis) is important for rotating your arm inwards, for example, when reaching across your front or reaching round into your back pocket. Tendon heals slower than bone and so certain movements will be protected after surgery to allow this tendon to heal. The healing of subscapularis back onto the bone is absolutely critical to the success, or otherwise, of the shoulder replacement.
The top image is a schematic diagram showing a total shoulder replacement with the poly-ethylene socket. The lower image is how the replacement appears on an X-ray. The socket is hardly visible because it is plastic and that doesn't show up on X-ray. In order that we can at least tell it is there and in the right place, a small piece of metal is embedded within the anchor-peg. This appears on the X-ray as a small line.
  SURGERY FOR THE SHOULDER WITH ARTHRITIS AND ROTATOR CUFF TEARA relatively new phenomenon in shoulder replacement surgery is the reverse shoulder replacement (RSA). Whilst the idea has been around for a few deacades, it has only really been popularised in the UK in the last 10-15 years as techniques and implants have improved. Recent data from the National Joint Registry showed that more reverse shoulder replacemenets are now being implanted than traditional anatomic replacements. The indications for an anatomic replacement has become narrower over time.
Instead of the ball being on top of the humerus and the socket being on the shoulder blade (anatomic), the positions are reversed so the socket is on the top of the humerus and the ball is mounted on the shoulder blade (reverse). The shoulder doesn't look any different from the outside of the body. This has huge benefits for the deltoid muscle in that the fulcrum (centre of rotation) is moved to make the muscle work more effectively. Of course, the deltoid is the only remaining functioning muscle since the rest of the rotator cuff has torn when this operation is considered.
This operation can lead to a patient regaining reasonable above-the-shoulder movement and a huge improvement in their pain. It should be noted however that the procedure is for pain-relief and it tends to do this quite reliably. It is not so reliable or predictable at restoring function. It may be that the function (movement) of the arm after RSA is the same as pre-operatively. The replacement can also be used if a patient has a poor result following a shoulder fracture and the rotator cuff becomes defunctioned because the lumps of bone which the tendons attach to are no longer in the correct position (see section on shoulder trauma).
The upper image shows an X-ray with arthritis secondary to a rotator cuff tear. The lower image shows a reverse shoulder replacement in situ with the fixed ball (hemisphere) attached with screws to the scapula (shoulder balde) and the socket on the top of the humerus. It's all stainless steel except the liner of the socket which is plastic, so you can't see it on the X-ray.
Spire Elland HospitalElland Lane
Elland
HX5 9EB
For an appointment, telephone:
Clinic bookings on 01422 324 069
Self pay enquiries on 01422 229 597
Main Hospital on 01422 229 632
BMI The Huddersfield Hospital
Birkby Hall Road
Huddersfield
West Yorkshire
HD2 2BL
Reception: 01484 533 131
Department of Orthopaedics & Trauma
Calderdale and Huddersfield NHS Foundation Trust
Huddersfield Royal Infirmary
Acre Street
Lindley
Huddersfield
HD3 3EA
NHS Secretary:
Mrs Margaret Thomas
Tel 01484 342 343
NHS Clinics Trauma:
Calderdale Royal Hospital (Halifax) and
Huddersfield Royal Infirmary
Elective Shoulder and Elbow problems:
Friday morning at Calderdale Royal Hospital, Halifax
|